

Numerous dental materials have come and gone over the past years. Many of their manufacturers have laid claims to a pure nonmetal aesthetic material with superior enamel-like strength. That’s like saying your dental practice provides the best service and the highest quality at the lowest price. The incongruence in that statement says it all.
I’d like to introduce to you Emax from Ivoclar. The material is lithium disilicate. The newest version of Emax is a high translucency (HT) ingot that provides fantastic aesthetic color depth with high mechanical strength. IPS Emax is an innovative all-ceramic system that covers the spectrum for indications throughout the entire mouth. In a recent study at New York University School of Dental Medicine, the flexural strength of 440mpa exceeds that of porcelain-to-zirconia restorations. The aesthetics of lithium disilicate has been improved with the high translucency ingot, which yields impeccable results along with incredible toughness to fracture.
Case Presentation

For this case, a 29-year-old female with a history of eating disorders was treated. She had conquered the illness, but the constant purging of stomach acidic fluids had eroded significant tooth structure, leaving the daily functions of eating, communicating, and smiling very unpleasant. The logistics of purging fluids from the mouth funnel the acids against the lingual surfaces of the maxillary teeth and create an erosion of tooth structure to a thin incisal edge. The incisal edges fracture under functioning and then thin out again until there is only half or less of the tooth left. Vertical dimension continues to change, and the whole stomatognathic system is disrupted.
 As viewed in the occlusal full-arch photo, severe erosion is noted. The ability of the patient to eat with a high concentration of sharp, occlusal articulation points of contact is difficult. The timing and force of her articulating surfaces are skewed, spelling out continued fracturing and discomfort. Aesthetics was the patient’s primary concern, with occlusal function a close second.
As viewed in the occlusal full-arch photo, severe erosion is noted. The ability of the patient to eat with a high concentration of sharp, occlusal articulation points of contact is difficult. The timing and force of her articulating surfaces are skewed, spelling out continued fracturing and discomfort. Aesthetics was the patient’s primary concern, with occlusal function a close second.
Procedure

The first and foremost important factor for this case was the physiologic rest position for the patient. Establishing a new vertical dimension will dictate the outcome for proper phonetics and proportions for an aesthetic result. Biopak information can be used for centric relation and/or musculature evaluation of vertical dimension and trajectory for masticatory function. Biopak is instrumentation used to establish vertical dimension.

Full-mouth models were taken using the Borderlock trays from Acculiner. These trays are strong with no flexing and capture great detail of the hamular notches and vestibules.
Preparation
 Practitioners are frequently hesitant to prep full arches due to the lack of a thought out plan. The results can vary dramatically due to no formulated structure for prepping and maintaining the vertical dimension of the existing bite or new diagnostic bite. The bite jig technique used in this case to maintain her new vertical dimension was fabricated from her mounted pre-op models. Prepping sequence is vital for efficiency when prepping full arches. Effective reduction and visualization for the practitioner to prep will allow the dental auxiliary to maintain her position whereby enhancing speed and reducing fatigue for the patient.
Practitioners are frequently hesitant to prep full arches due to the lack of a thought out plan. The results can vary dramatically due to no formulated structure for prepping and maintaining the vertical dimension of the existing bite or new diagnostic bite. The bite jig technique used in this case to maintain her new vertical dimension was fabricated from her mounted pre-op models. Prepping sequence is vital for efficiency when prepping full arches. Effective reduction and visualization for the practitioner to prep will allow the dental auxiliary to maintain her position whereby enhancing speed and reducing fatigue for the patient.

The example of prepping a lower arch starts by prepping the right quadrant. Prep teeth 27–30. Always leave the most distal tooth, giving the dentist an occlusal stop.
Prepping Steps
 330 carbide to open contacts.
330 carbide to open contacts.- 330 carbide to reduce occlusal height.
- Prep #30 with 5856 diamond at the axial walls starting distally and moving counterclockwise to mesial, then stop and move to next tooth until you reach tooth 27. This prepping is to full contour.
- Prep lingual of tooth #27 and move to next tooth until you reach #30.
 Occlusal reduction and round all sharp edges.
Occlusal reduction and round all sharp edges.- Use stent reduction guide to verify proper form and contours.
- Prep left side same way teeth #22–20 (tooth 19 most distal stop).
- Insert bite jig and have patient practice closing fully into matrix bite jig. Measure with boley gauge cervical margin of #8 to cervical margin of #25.
 Apply regisil bite paste to prepped areas 20–22 and 27–30. Insert bite jig and have patient close fully into it. Verify vertical dimension with boley gauge measuring from tooth 8–25.
Apply regisil bite paste to prepped areas 20–22 and 27–30. Insert bite jig and have patient close fully into it. Verify vertical dimension with boley gauge measuring from tooth 8–25.- Complete prepping of remaining teeth 19, 23–26, and 31. Spot in registration paste being careful not to spill into previous relined areas.



When prepping for Emax restorations, always create a well-defined solid shoulder prep. Featheredge preps are contraindicated for Emax restorations.
Cementation Delivery
IPS Emax restorations can be placed using adhesive or self-adhesive and conventional techniques. The sequence for cementing a full arch after try in of all restorations goes as follows:
 Cement posterior molars. Start with right side, cementing molars with multilink automix from Ivoclar. Allow for proper curing time before placing rubber dam clamps on molars.
Cement posterior molars. Start with right side, cementing molars with multilink automix from Ivoclar. Allow for proper curing time before placing rubber dam clamps on molars.- Place rubber dam and seal off palate.
- Cleanse teeth, rinse, and lightly dry.
- Acid etch teeth, rinse, and lightly dry.
- Apply Systemp desensitizer from Ivoclar, and lightly dry.
- Apply multiple coats of adhesive to tooth structure.
- Apply Variolink veneer cement to veneer.
- Place restorations shy of fully seating.
- Fully seat one restoration at a time a spot tack cure at gingival margin for 2 seconds then continue to next tooth, tack cure, and so on. Once all restorations are tack cured, gently wipe away excess cement from the lingual surface with a cotton roll starting incisally toward the gingival margin. Visually check the lingual margin to assess full seating of restorations.
- Wave cure over all restorations for 2 seconds. Gently remove excess cement. Apply de-ox (oxygen inhibitor) from Ultradent at the margins. Fully light cure for 20 seconds.
- Remove all cement and floss interproximally.
- Finalize occlusion in 48 hours using a Tekscan for time and force.

Conclusion
 A literature review of longevity and clinical performance of IPS Emax restorations revealed favorable clinical results. Guesss investigated the survival rate and long-term behavior of all-ceramic restorations on molars. Pressed ceramic Emax and CAD/CAM Emax were compared. Clinical recall at 28 months after luting with a light polymerized resin cement showed a 97 percent survival rate for the Emax CAD and 100 percent for Emax pressed. The clinical accuracy of the marginal fit for both Emax CAD and Emax press were excellent.
A literature review of longevity and clinical performance of IPS Emax restorations revealed favorable clinical results. Guesss investigated the survival rate and long-term behavior of all-ceramic restorations on molars. Pressed ceramic Emax and CAD/CAM Emax were compared. Clinical recall at 28 months after luting with a light polymerized resin cement showed a 97 percent survival rate for the Emax CAD and 100 percent for Emax pressed. The clinical accuracy of the marginal fit for both Emax CAD and Emax press were excellent.
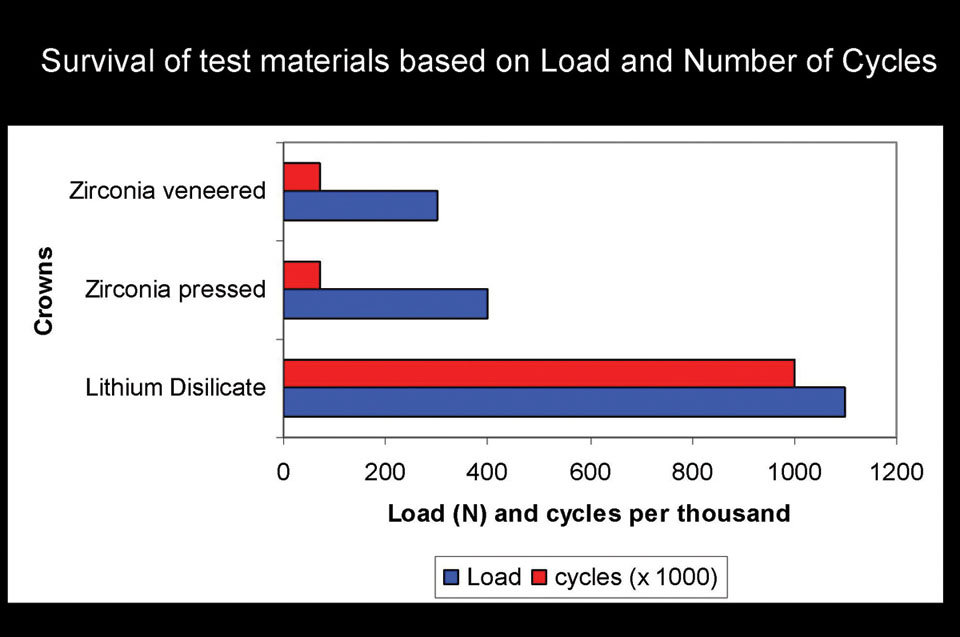
 Lithium disilicate is becoming the restorative material of choice when it comes to single-unit indirect restoration. Full-contour posterior crowns fabricated out of Emax CAD offers 360 mpa of strength throughout the whole crown, which demonstrates the “monolithic” strength unlike any other metal or metal-free crown. When comparing studies of strength (mpa) to porcelain fused to matel (80–100 mpa) or porcelain veneered to zirconia (100 mpa) and leucite glass
Lithium disilicate is becoming the restorative material of choice when it comes to single-unit indirect restoration. Full-contour posterior crowns fabricated out of Emax CAD offers 360 mpa of strength throughout the whole crown, which demonstrates the “monolithic” strength unlike any other metal or metal-free crown. When comparing studies of strength (mpa) to porcelain fused to matel (80–100 mpa) or porcelain veneered to zirconia (100 mpa) and leucite glass










