

Go from “Practicing” to Providing the Right Solution.
Shawn and I became friends when we were children and we had the good fortune of staying friends into adulthood. When I was in dental school, Shawn mentioned that someday he would like me to look at some problems he was having with his teeth. The operative word, I might add, was “someday.” As an eager dental student, I encouraged Shawn to come in right away so I could resolve his issues immediately. “Why wait? Let’s do this now!” I said. However, Shawn was cautious. He didn’t want me to “practice” on him while I was still a student, but he said he would definitely come in for a visit once a diploma hung on my wall. That truly was a brilliant move on Shawn’s part because the dentistry that Shawn really needed—and that I was finally able to complete for him—was definitely not the type of dentistry that I could do while still in school.
Shawn’s First Visit
After graduation from dental school, I began my career at a corporate office. After a few months of practicing there, Shawn made his first appointment. Shawn has never been a big complainer about anything—but when we chatted about his dental issues, I learned that there were some major issues in his mouth that were causing him serious discomfort. He mentioned that his teeth were extremely sensitive. He also had some concerns with two of his lower molars that were giving him additional pain. His jaw was also constantly sore. Shawn often woke up in the middle of the night and had difficulty getting a good night’s sleep. In the morning, he usually experienced severe pain in his head, face, and neck. When Shawn explained everything, I remember thinking, ‘It would be terrible to feel that way every single morning.’
As I examined Shawn’s mouth, I discovered part of the problem. Shawn had a flat plane of occlusion that was just about edge-to-edge, with very little enamel left on the occlusal surfaces. He had no cuspid guidance and had worn the posterior enough to lock in the lower incisors. Through the years, due to the wear, as he would clench his jaw he would over-close and compress his disc and retrodiscal tissue, causing frequent pain. The lack of healthy intercuspation in centric relation also caused muscle spasms in the pterygoids. His lower first molars had decay near the pulp. In addition, Shawn’s masseter muscles were absolutely massive. He was likely using those muscles all day long. Those particular muscles were extremely sensitive to the touch, as were his temporalis muscles. In short, he was a dental mess.
At the time, the best course of action was to directly address the issues Shawn was having with his first lower molars. I honestly thought that if I put a strong material on the teeth, it would prevent Shawn from bruxing. My idea was to use Ivoclar’s blue blocks CEREC e.max crowns because they were supposed to be as hard as rocks. I thought that Shawn could hardly grind his way through those. I completed the procedure and naïvely thought that my dental solution would be an immediate resolution for Shawn’s problems.
Well, the longer I am in the field of dentistry, the more I realize that every case—every person—is completely and totally unique. The blue block crowns didn’t work at all for Shawn. He was glad to have the work done, of course, but his teeth clenching continued just as before, and his headaches and tension were still prevalent.
Introduction to Advanced Dentistry
A few months later, I left the corporate practice and purchased an established practice that was run by what I like to call a “Barnesified” dentist. The dentist was educated by the Dr. Dick Barnes Group, and over the years he applied that knowledge to his practice, which became very successful. As a result, the veteran dentist performed all kinds of advanced dental procedures to give his patients optimal care—including surgery, implants, orthodontics, and cosmetic dentistry.
Yet at the time, I was doing none of those things! I spent four years in dental school and about half a million dollars to learn about the mouth and how to prevent tooth decay, how to repair broken or decaying teeth, and how to replace teeth in general, but I wasn’t skilled enough to do any of the advanced procedures that this dentist was doing for his patients. Suddenly, I felt like I was in very deep water and barely staying afloat.
Soon after purchasing the practice, I received a surprise visitor. Dr. Dick Barnes was visiting offices and decided to stop by to see me—the rookie dentist who had just purchased the practice. During a lunch appointment, Dr. Barnes invited me to sign up for the “Over the Shoulder” Full Mouth Reconstruction course held at Arrowhead Dental Laboratory in Utah. He believed it would have such a transformation on my career, he invited me to attend the class as his special guest. Dr. Barnes said, “I want you to take this class. I want you to change your practice. I want you to step it up.”
I was impressed by Dr. Barnes’s generosity and the strong belief that he had in his courses. So I accepted his offer and signed up for the training. Dr. Jim Downs led the course and it was just as career changing as Dr. Barnes had described. As I sat in the course, learning about the many symptoms that full mouth reconstructions can resolve, I immediately thought about Shawn and the conditions that we had failed to resolve months earlier. A full mouth reconstruction would definitely benefit Shawn!
I was so energized that I didn’t want to wait until that evening to reach out to Shawn. While in class, I pulled out my phone and immediately texted him. I said, “I’ve got it! I’ve got the solution that will fix your problem!” I briefly explained to him some of the procedures that I had just learned and how I believed they would help his situation. He texted back an affirmative message: “Let’s do it!” he said. I have to admit that I think Dr. Barnes would be particularly impressed that my first full arch case presentation—conducted entirely via text message—was not only well received, it was unequivocally accepted!
The Work Begins
 When I returned to my office, I immediately began working on Shawn’s full mouth reconstruction. The first step was splint therapy. Since Shawn ground his teeth down so significantly, he had lost vertical dimension. I decided to use splint therapy as an inexpensive and reversible way to prep the patient for permanent jaw realignment. With a splint, we adjusted the vertical dimension and tested for comfort.
When I returned to my office, I immediately began working on Shawn’s full mouth reconstruction. The first step was splint therapy. Since Shawn ground his teeth down so significantly, he had lost vertical dimension. I decided to use splint therapy as an inexpensive and reversible way to prep the patient for permanent jaw realignment. With a splint, we adjusted the vertical dimension and tested for comfort.
Before splint therapy, Shawn had a Shimbashi (measurement from CEJ of upper central to lower central) of 16 mm, edge to edge. After conducting a few tests, I found that Shawn was most comfortable at a 19 mm Shimbashi. We built the splint around that Shimbashi goal and I instructed Shawn to wear the device every night and as often as possible during the day.
After just a week of wearing the splint, Shawn reported, “My headaches are gone and I can sleep all night!” The splint made such a positive impact on his overall comfort level that he started wearing the device all day long instead of just at night. Shawn continued to wear the splint for the next three months and we adjusted it every couple of weeks, as needed.
This “time test” for splint therapy is a crucial part of a full arch case, especially with patients who are bruxers like Shawn. Before you do anything permanent, the Shimbashi should be dialed in. Also, make certain that the clenching is gone and that the muscle sensitivity is reduced or eliminated.
With a guy like Shawn, who has strong masseter muscles and a major tooth-grinding habit, I had to ensure that the tooth-grinding issue was resolved before I fitted him for porcelain teeth. After all, his “mad chops” and a set of “glass” teeth were definitely not a good combo!
When splint therapy was complete, we ordered the white wax-up and scheduled Shawn for his prepping appointment. Because Shawn was my first full mouth case, I didn’t want to attempt prepping both arches at once. On the day we prepped the upper arch, I drove him to the office, made him comfortable with his favorite music on some headphones, inserted the Isolite, and began to prep the teeth.
Because we were opening his bite, I didn’t need to prep very much. In the wax-up phase, we widened his upper arch with my preps. We wanted more tongue space and buccal support, so I mainly prepped the palatal and just parallelized the buccal. We didn’t want to constrict the lower, since our goal was to increase tongue space for better breathing purposes.
We did that by making sure the upper temps fit nicely to the lowers. Typically, changing the top to an ideal when you still have a lower that is non-ideal will cause occlusal scheme issues and potential fractures. However, in Shawn’s case, we prepped the lowers immediately after cementing the uppers.
Since Shawn’s case, I have prepped the upper and lower arches at the same time. Another possibility, if prepping both arches at the same time is not an option for the patient (because of financial reasons or other issues), is to put the lowers in overlay-style temps like Arrowhead’s Radica® (Snowcaps). This buys time for the patient and can be helpful for people who need to save money before restoring both arches.
I made a single unit temp for Shawn. Without any adjustment, it was perfect! The fit was amazing, as was the bite. Shawn was in his full upper temp for over a month.
Shawn was extremely impressed with his transformation, even after getting just his temps. Besides wanting to have his teeth restored for functional and health reasons, Shawn also wanted a more attractive smile. I think most people have that dream. About every other day after Shawn received his temps, he texted me, saying, “I can’t believe how great these look! Thank you, buddy!” He was non-stop in his enthusiasm for his new smile—and those were just the temps! Honestly, the temps make most people look like a supermodel compared to what they looked like before. Shawn definitely looked, felt, and acted like a different person.
A Permanent Smile
For Shawn’s permanent smile, we used e.max press crowns on all but the second molars and full gold on his second molars. We chose to use gold on this set of molars as a solid stop. I also fitted Shawn with a new nocturnal orthotic to protect his new set of beautiful Elite crowns from any possible nighttime bruxism habits that remained.
At bonding, I noted that Shawn was meticulous with rinsing, because his gums were pink with very little inflammation. Had he not cared for his temps in such a dedicated fashion, I most likely would not have been able to bond a full upper set due to bleeding. The try-in was magical and the fit was unreal. Each crown slid into place from front to back with ease. The bite was just as precise as it had been with the temps.
I cemented the gold second molars first to establish the bite and then I moved forward in the mouth from there. The process moved so smoothly that we actually decided to prep and seat the lower arch in the same visit. That’s the benefit of having the full case waxed up and the Sil-Tech® temp guides for the upper and lower arches. We had them in the office, so it was no problem to move to the other arch. The process went just as smoothly with the lowers as it did with the uppers.
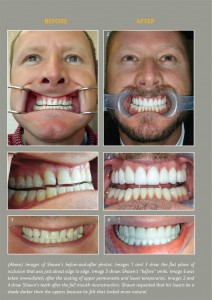
By the end of the visit, Shawn had his brand new smile. He was in love. I was also extremely impressed with the natural look of the teeth. The translucency of the anteriors surpassed any of my expectations. The teeth weren’t just good looking, they matched his facial profile.
After seeing how Shawn reacted to his temps, I knew that Shawn’s reaction to his permanent smile would be positive. But I was truly surprised at how moved he was the first time he saw his smile with his new Elite crowns. Shawn is not a very emotional person. So when I saw his reaction, I was a little taken aback. He was actually moved to tears. He was so overwhelmingly happy with the results of the entire process. Not only did we address his health problems with the full arch procedure, but he also had this great smile as an added bonus. It was something that he had never even thought of as a possibility—something he never dreamed would happen. He then asked me to do the same treatment for his girlfriend.
Now Shawn smiles constantly. He smiles because he feels great. And he smiles because he has a great smile! He’s also far more confident at his job. That confidence has literally paid Shawn back in many ways—including in his finances. When I asked Shawn if he’s made more money since having his teeth done, he said, “Absolutely!” Shawn’s finances increased because of a corresponding increase in confidence and ambition levels. Also, Shawn has been more successful in his career because he feels better. He’s sleeping better and he has no pain from headaches or tense facial and jaw muscles. As is the case for most people, when you feel better, your entire life dramatically improves.
Moving Forward
 Shawn’s case has impacted my life tremendously as well. If I hadn’t taken the full arch reconstruction course and learned about the possibilities of full mouth reconstruction, I’m not sure where my career would be today. It has caused my career to take off in a very positive direction. I’ve completed many full arch cases since Shawn’s and I plan to do many more in the future.
Shawn’s case has impacted my life tremendously as well. If I hadn’t taken the full arch reconstruction course and learned about the possibilities of full mouth reconstruction, I’m not sure where my career would be today. It has caused my career to take off in a very positive direction. I’ve completed many full arch cases since Shawn’s and I plan to do many more in the future.
Shawn isn’t the only person who is smiling now. So am I! So is my team! And so are all of the patients who are benefiting from the advanced dentistry that I now proudly offer in my practice!
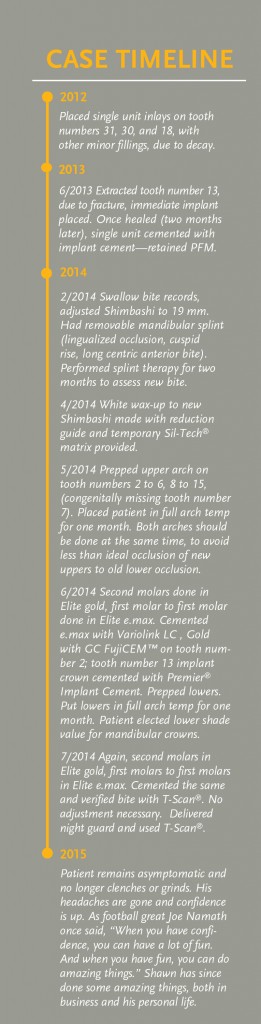
CASE TIMELINE
2012
- Placed single unit inlays on tooth numbers 31, 30, and 18, with other minor fillings, due to decay.
2013
- 6/2013 Extracted tooth number 13, due to fracture, immediate implant placed. Once healed (two months later), single unit cemented with implant cement—retained PFM.
2014
- 2/2014 Swallow bite records, adjusted Shimbashi to 19 mm. Had removable mandibular splint (lingualized occlusion, cuspid rise, long centric anterior bite). Performed splint therapy for two months to assess new bite.
- 4/2014 White wax-up to new Shimbashi made with reduction guide and temporary Sil-Tech® matrix provided.
- 5/2014 Prepped upper arch on tooth numbers 2 to 6, 8 to 15, (congenitally missing tooth number 7). Placed patient in full arch temp for one month. Both arches should be done at the same time, to avoid less than ideal occlusion of new uppers to old lower occlusion.
- 6/2014 Second molars done in Elite gold, first molar to first molar done in Elite e.max. Cemented e.max with Variolink LC , Gold with GC FujiCEM™ on tooth number 2; tooth number 13 implant crown cemented with Premier® Implant Cement. Prepped lowers. Put lowers in full arch temp for one month. Patient elected lower shade value for mandibular crowns.
- 7/2014 Again, second molars in Elite gold, first molars to first molars in Elite e.max. Cemented the same and verified bite with T-Scan®. No adjustment necessary. Delivered night guard and used T-Scan®.
2015
- Patient remains asymptomatic and no longer clenches or grinds. His headaches are gone and confidence is up. As football great Joe Namath once said, “When you have confidence, you can have a lot of fun. And when you have fun, you can do amazing things.” Shawn has since done some amazing things, both in business and his personal life.








